Cart
×

Kevin Flanigan, MD is a leading expert in the development of gene therapies for Duchenne, and the director of the Center for Gene Therapy in the Abigail Wexner Research Institute at Nationwide Children’s Hospital. Recently, Dr. Flanigan and his team made a “landmark announcement” where they successfully produced full-length dystrophin protein in the muscle of Duchenne patients following exon-skipping therapy. This result marks a long-awaited milestone in Duchenne research and offers hope for a significant number of Duchenne patients with very rare mutations.
Dr. Flanigan’s work on gene therapy for Duchenne began more than a decade ago. When CureDuchenne founder and CEO Debra Miller met with him in 2010, she believed strongly that this research had the potential to move the needle towards a cure for some Duchenne patients. At the time, the research was at a very early preclinical stage. It aimed to solve the problem of exon duplications, which itself represents a subset of mutations in an already rare disease.
Debra’s vision of supporting and de-risking promising science would if successful, help accelerate the search for meaningful treatments for people living with Duchenne. Research like this carries significantly more risk and treats fewer patients. For this reason, it is not always conducted at pharma and biotech companies.
CureDuchenne gathered resources to help move Dr. Flanigan’s work forward in 2010 to initially fund the creation of a new mouse model with an exon 2 duplication. Later, in 2014 and again in 2017, CureDuchenne continued funding this work through the pre-clinical phase of development. In total, CureDuchenne supplied $1 million between 2010 and 2017 to support Nationwide’s duplication exon 2 gene therapy treatment.
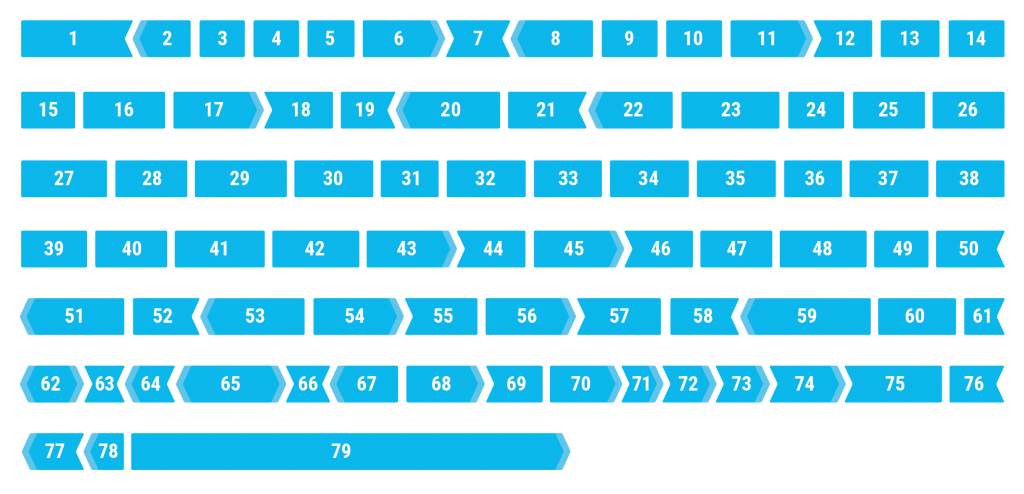
For a quick genetics refresher – genes are divided into exons, sections of DNA that code for protein. Dystrophin is our largest gene and contains 79 coding exons. An error in processing the information contained in any exon could be pathogenic and lead to some form of muscular dystrophy, Duchenne being the most severe. Errors can be in the form of deletions, duplications, point mutations, and other forms.
Duplications of exons account for an estimated 10% of all mutations in Duchenne. Until this work, therapeutic approaches generally neglected duplications. The most common duplication-related form of DMD (affecting about 1% of all people with DMD) involves an extra copy of exon 2. This mutation disrupts the reading frame and causes cells to stop making dystrophin protein.
It’s worth noting that while this specific mutation is the most prevalent disease-causing duplication, just a few hundred people may be amenable to treatment using Nationwide’s exon-skipping approach. Importantly, the success of this research has implications beyond solving a problem for a single exonic duplication.
Dr. Flanigan’s research lab identified a new Internal Ribosome Entry Site (IRES) in the dystrophin gene on exon 5. This offers a larger therapeutic window for skipping duplicated exon 2 by initiating translation of the dystrophin protein at exon 6 onwards if the 2nd copy of the exon was skipped. Put simply, skipping one copy of the duplicated exon 2 produces natural full-length dystrophin, and skipping both copies activates the IRES on exon 5 to produce a slightly shorter, truncated, highly functional dystrophin protein lacking the first 5 exons.
The latest clinical results are nothing short of outstanding. In a 7-month-old Duchenne patient, a muscle biopsy showed that 99% of his muscle fibers produced full-length dystrophin after a single treatment with the exon 2 skipping drug.
CureDuchenne has been on a hunt for therapies that could generate full-length dystrophin protein as a solution for everyone living with Duchenne. These results provide support for the usefulness of this approach to treating patients with duplications of exon 2 and a potential treatment option for mutations within the first 5 exons of the dystrophin gene. The ability to safely deliver treatments at a very young age could also transform the current landscape of therapeutics for muscular dystrophy.
One more very important takeaway for the greater Duchenne population is the importance of newborn screening. With positive results on a 7-month-old, newborn screening may be even more important than we previously knew. CureDuchenne’s pilot program at Brigham and Women’s Hospital was the first program to offer supplemental newborn screening for Duchenne in a clinical setting. Researchers and clinicians have worked for 20 years toward a genetic screening for Duchenne, yet the average age of diagnosis remains at about four years old. CureDuchenne will continue pushing to make Duchenne genetic testing more widely available so future generations can realize better outcomes from early intervention.
We’re very grateful for all the backing from our donors and partners who supported our venture philanthropy model. This allows us to fund groundbreaking research, early diagnosis and treatment access for individuals with Duchenne.